






Echoendoscopic fine-needle aspiration puncture
Echoendoscopic fine-aspiration puncture
Endoscopic ultrasound fine-needle aspiration (EUS-FNA, endoscopic ultrasound fine needle aspiration) is an established tissue acquisition technique for various indications, especially for solid and cystic pancreatic lesions, but also for access for some interventional procedures.
Since the first ultrasound endoscopic puncture, performed in 1992 by Prof. Peter Vilmann, both ultrasound probes and puncture needles have experienced accelerated progress, so that “histological needles” are now available, which allow fine-bioptic puncture.
Before performing the echoendoscopic puncture:
- establishing the indication of fine-aspiration puncture
- evaluation of antithrombotic medication (EUS-FNA is defined as a “high-risk” procedure in the ESGE guidelines)
- checking coagulation tests and platelet counts, correcting coagulopathy at INR > 1.5, platelets < 50,000/mm3
the choice of the puncture needle (function of the type of lesion, localization, hemorrhagic risk, the amount of material required for diagnostic tests – - cytology/histology/immunohistochemistry)
- ensuring the sedation of the patient in parallel with the monitoring of vital signs
Echoendoscopic puncture technique
- The lesion to be punctured is positioned near the transducer
- The presence of vasculature in the path of the puncture needle is verified by using the Doppler mode
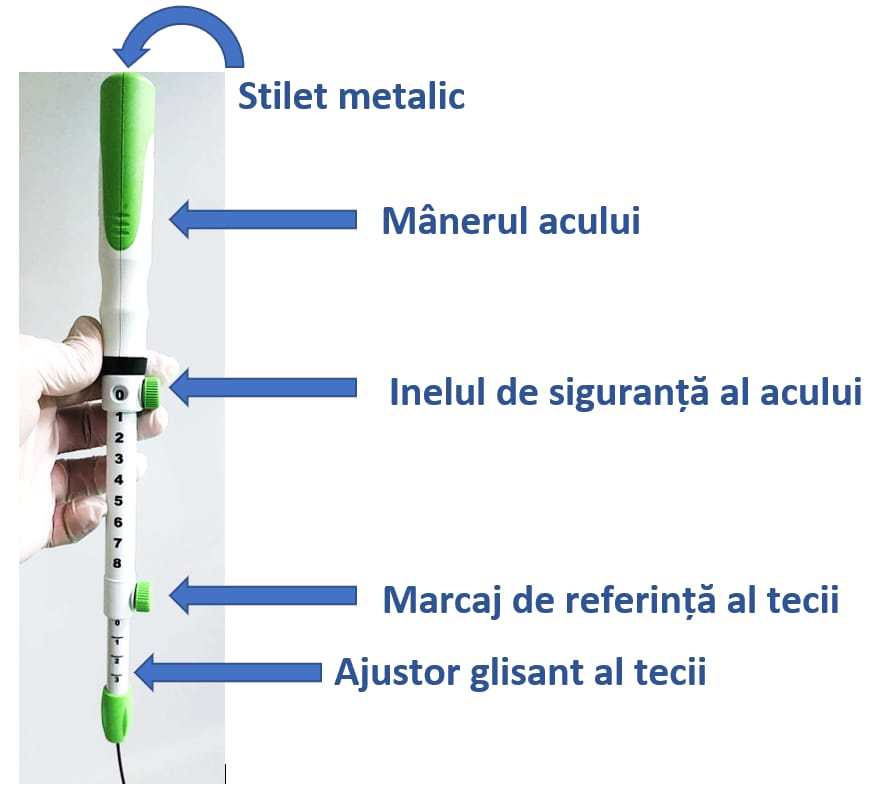
- Check the positioning of the reference mark of the sheath at the “0” position and of the safety ring of the needle at “0” – Figure 1.
- The valve is removed from the level of the working channel of the echoendoscopy probe
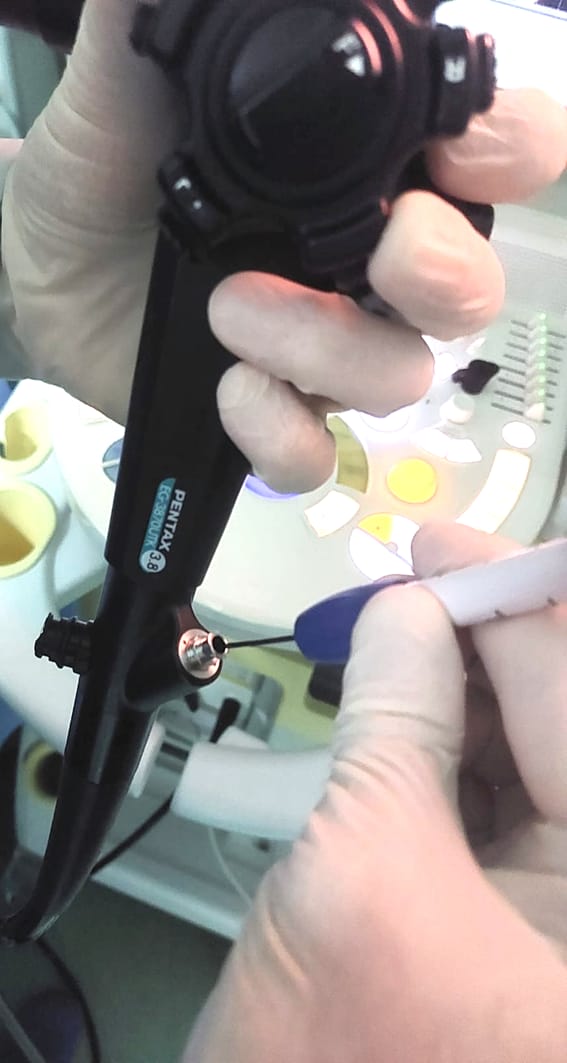
- The needle is inserted through the working channel of the echoendoscope and advanced until the coupling system at the base of the sliding sheath adjuster reaches the level of the metal end of the working channel, then it is screwed and fixed – Figure 2 and 3.
- Adjust the desired sheath length by loosening the screw on the sheath slide adjuster and sliding down to the desired length. The needle sheath will be visible on the endoscopy and ultrasound image. After moving the reference mark to the desired length, tighten the screw on the sheath sliding adjuster to fix the selected length – Figure 4 and 5.
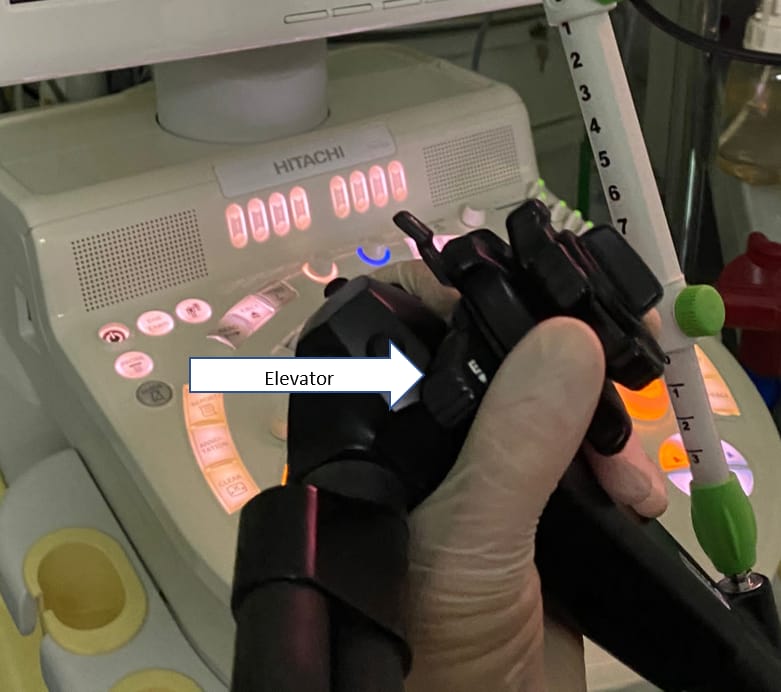
- Recheck the position of the lesion on the ultrasonographic image and adjust the puncture path by using the elevator on the echoendoscopy probe – Figure 6.
- Loosen the rotator screw on the needle safety ring and either lower it completely or tighten (by tightening the screw) to the desired needle advance reference mark. The number in the safety ring window will represent the extension of the needle in centimeters. The lesion is punctured by advancing the needle handle and “go/come” movements are performed in the lesion, simultaneously with the progressive withdrawal of the stylet from the needle (pulling the distal end visible on the needle handle) – Figure 7, 8, 9.
- When the puncture is complete, withdraw the needle into the sheath by withdrawing the needle handle and locking the screw on the safety ring at position 0 – Figure 10.
- Disconnect the needle device from the accessory channel of the echoendoscope, withdraw it completely, and then express the collected material from the puncture needle.
Particularities of the technique
In addition to the technique illustrated above, with the progressive withdrawal of the stylet (slow-pull), there is also the possibility of using a suction syringe (suction technique) or pre-washing the needle with physiological serum and suction (wet-suction technique). Regarding the puncture maneuver, variants such as “door-knocking” or “fanning” (the fan technique) are described.
References:
- Vilmann P, Jacobsen GK, Henriksen FW, Hancke S. Endoscopic ultrasonography with guided fine needle aspiration biopsy in pancreatic disease. Gastrointest Endosc. 1992;38(2):172-173. doi:10.1016/s0016-5107(92)70385-x
- Veitch AM, Radaelli F, Alikhan R, et al. Endoscopy in patients on antiplatelet or anticoagulant therapy: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guideline update. Gut. 2021;70(9):1611-1628. doi:10.1136/gutjnl-2021-325184
- Kovacevic B, Vilmann P. EUS tissue acquisition: From A to B. Endosc Ultrasound. 2020;9(4):225-231. doi:10.4103/eus.eus_21_20
- Cazacu IM, Luzuriaga Chavez AA, Saftoiu A, Vilmann P, Bhutani MS. A quarter century of EUS-FNA: Progress, milestones, and future directions. Endosc Ultrasound. 2018;7(3):141-160. doi:10.4103/eus.eus_19_18
- Dumonceau JM, Deprez PH, Jenssen C, et al. Indications, results, and clinical impact of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline – Updated January 2017. Endoscopy. 2017;49(7):695-714. doi:10.1055/s-0043-109021
- Polkowski M, Jenssen C, Kaye P, et al. Technical aspects of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Technical Guideline – March 2017. Endoscopy. 2017;49(10):989-1006. doi:10.1055/s-0043-119219
- Dietrich CF, Arcidiacono PG, Braden B, et al. What should be known prior to performing EUS?. Endosc Ultrasound. 2019;8(1):3-16. doi:10.4103/eus.eus_54_18
- Dietrich CF, Arcidiacono PG, Braden B, et al. What should be known prior to performing EUS exams? (Part II). Endosc Ultrasound. 2019;8(6):360-369. doi:10.4103/eus.eus_57_19