











More than meets the eye – a clincal case
A 76 year old female patient presented in the Gastroenterology department of Colentina Clinical Hospital in January 2022 for recurrent abdominal pain and involuntary weight loss of about 9kg în the past 3 months.
In 2021 she had presented 2 episodes of acute pancreatitis of unknown cause, alcohol abuse and biliary stones being excluded at that moment. Her medical history includes, arterial hypertension, ischemic cardiomyopathy and severe aortic stenosis for which corrective surgery was proposed but which the patient had declined.
At the present evaluation the clinical examination was unremarkable except for a murmur of the aortic stenosis.
At the current work-up, the patient had cholestasis (GGT 252UI/L, FAL 215 UI/L) and a mild inflammatory syndrome (CRP 7mg/L) with no other notable findings.
A recent abdominal CT scan with intravenous contrast described dilatation of the distal common bile duct (CBD) of approximately 7.5 mm as well as a 6 mm nodular lesion at this level suggestive of choledocolithiasis.
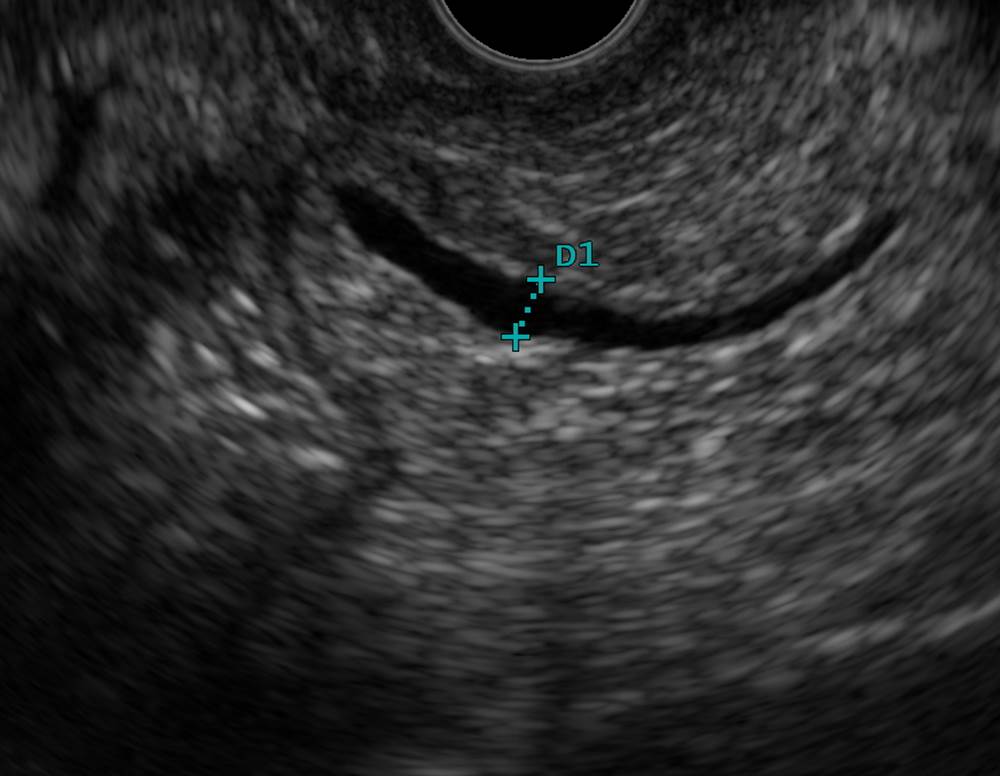
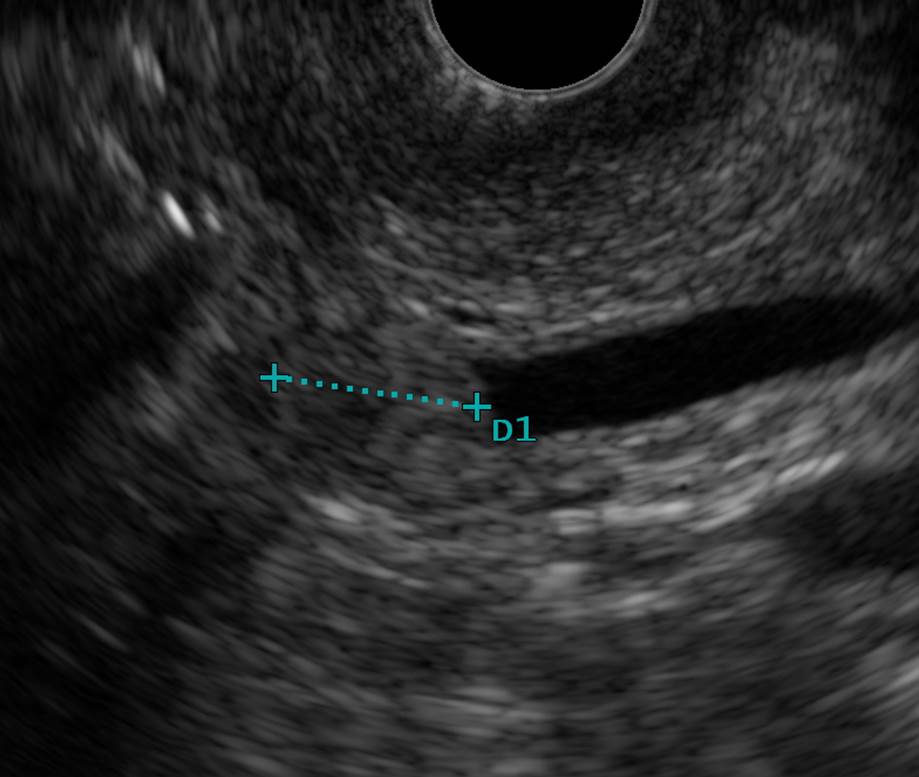
An endoscopic ultrasound (EUS) was performed in order to characterize the common bile duct (CBD) and the head of the pancreas: the pancreatic parenchyma seemed slightly heterogenous, with an inflammatory aspect; the Wirsung duct measured 3.2 mm, it had relatively irregular, hyperechoic walls (Figure 1); the distal CBD measured 7.5 mm and it had thick walls (Figure 2). A hypoechoic lesion, with no posterior acoustic shadowing, was detected inside the distal CBD, just above the ampullary region, suggesting an intraductal polyp. We then continued the evaluation with an endoscopic retrograde cholangiopancreatography (ERCP): the papilla had a modified mucosa over an area of about 1 cm2 , compatible with an ampulloma at white light and methylene blue chromoendoscopy examinations (Figure 3). The cholangiogram showed a minimal CBD dilatation of approximately 7 mm, with a short distal stricture, compatible with an ampulloma with intraductal extension (Figure 4). Given the suspicion of an intraductal component of the lesion, we decided to perform an intraductal ultrasound evaluation to determine the extension of the lesion – it measured about 5 mm and showed no signs of invasion beyond the biliary wall (Figure 5). We obtained papillary biopsies and placed a 7Fr/7cm CBD stent, without sphincterotomy in order to avoid compromising the possibility of an subsequent endoscopic resection (Figure 6).
The pathology report of the ampullary biopsies confirmed the presence of a tubular adenoma with minimal villous component, with low grade neoplasia (Figure 7).
In February 2022, the patient was admitted for a scheduled endoscopic papillectomy after declining surgical treatment. Selective cannulation of the Wirsung duct using a guidewire and a sphincterotome was initially performed, followed by injection of a solution of contrast agent and methylene blue (in order to facilitate selective cannulation of the pancreatic duct after the resection). Hot snare resection a 15 mm snare was performed and a pancreatic stent (5Fr/3cm) was then placed in the Wirsung duct (Figure 8). The patient developed a mild episode of acute pancreatitis, which was quickly resolved with conservative treatment. The histopathology report confirmed the presence of adenoma fragments within the resection limit (Figure 9).
In April 2022 we reevaluated the patient who had a good clinical status. During ERCP we found the pancreatic stent and remnant adenomatous tissue, including a central depressed area suggesting a possible invasion in the distal CBD. We extracted the pancreatic stent, we performed an occlusion cholangiogram using a balloon demonstrating a short distal CBD stricture, we obtained biopsies and placed a 10Fr/5cm plastic biliary stent; the pathology report confirmed the presence of recurrent adenomatous tissue with low grade dysplasia.
According to the ESGE guideline [1], we decided to perform an additional endoscopic procedure (thermal ablation or intraductal radiofrequency ablation with temporary biliary stenting) to treat the remnant adenomatous tissue.
During ERCP we observed an enlarged papilla, with obvious adenomatous tissue of about 1 cm2 (Figure 10); we performed a selective cannulation of the CBD for a new cholangiogram (Figure 11) followed by a selective cannulation of the Wirsung duct and the placement of a 5cm/5Fr stent (Figure 12). Intraductal radiofrequency ablation using the Habib probe (10w/90s) in the distal CBD was performed (Figure 13), followed by the treatment of the remnant ampullary adenomatous tissue by plasma argon coagulation (40x, 0.6L/min) (Figure 14). Finally, a 5cm/10Fr CBD stent was placed to facilitate biliary drainage.
The postprocedural evolution was unremarkable and the patient was discharged in good clinical condition.
Particularity of the case. Discussions.
Ampullary adenomas with intraductal extension are usually referred for surgical therapy given the frequently incomplete endoscopic resection (complete resection in 46% versus 83% for no intraductal involvement) resulting in reintervention or even rescue surgery (37% versus 12%). [1] However, pancreaticoduodenectomy is associated with a high risk of morbidity and mortality, and in our patient’s case a minimally invasive iterative endoscopic treatment was preferred due to coexisting conditions. This novel therapeutic approach is supported by recent data proving a high success rate for papillectomy combined with radiofrequency ablation [2,3].
Referrals
[1] Vanbiervliet G, Strijker M, Arvanitakis M et al. Endoscopic management of ampullary tumors: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2021 Apr
[2] Pérez-Cuadrado-Robles E, Piessevaux H, Moreels TG, et al. Combined excision and ablation of ampullary tumors with biliary or pancreatic intraductal extension is effective even in malignant neoplasms. United European Gastroenterol J. 2019
[3] Tringali A, Matteo MV, Orlandini B, Radiofrequency ablation for intraductal extension of ampullary adenomatous lesions: proposal for a standardized protocol. Endosc Int Open. 2021 May;
Figure 1 Ultrasound image – Wirsung duct measuring 3.2 mm, with relatively irregular, hyperechoic walls;
Figure 2 Ultrasound image – distal CBD with relatively well defined, hypoechoic area – intraductal polyp;
Figure 3 Duodenoscopy – enlarged, modified papilla suggesting a possible ampulloma;
Figure 4 ERCP – contrast agent in CBD showing a minimal CBD dilatation with distal stricture;
Figure 5 Intraductal ultrasound image showing the 5 mm hypoechoic lesion belonging to the distal CBD;
Figure 6 ERCP – CBD stenting;
Figure 7 Tubular adenoma with minimal villous component – low grade intraepithelial neoplasia. HE, 100x (Courtesy of dr. Cristiana Popp, Department of Pathology, Colentina Clinical Hospital);
Figure 8 ERCP – pancreatic stent (red arrow);
Figure 9 Large area of electrocoagulation with small superficial areas from a tubular adenomatous proliferation with low grade dysplasia. HE, 100x (Courtesy of dr. Cristiana Popp, Department of Pathology, Colentina Clinical Hospital);
Figure 10 ERCP – enlarged papilla, with obvious remnant adenomatous tissue;
Figure 11 ERCP – cholangiogram – mild dilatation of CBD with distal stricture;
Figure 12 Pancreatic stent (red arrow);
Figure 13 Intraductal RFA on distal CBD using the Habib probe (10w/90s);
Figure 14 Plasma argon ablation (40w,0.6L/min) of the adenomatous tissue.